Stop the CCM Spreadsheet Nightmare.
CCM pays for the “between-visit” work your team already does--care coordination, patient outreach, and updating an electronic care plan--billed by the calendar month under general supervision of the billing practitioner.[1] FairPath automates time capture, enforces CMS stacking rules, and generates clean, auditable claims.
Calculate Your CCM Revenue See How We Automate Time-Tracking ↓Not sure about the specific CPT requirements? Read our Deep-Dive Guide to CCM Compliance.
CCM: Great for Patients, Brutal Without Automation.
CMS built CCM to reward longitudinal, team-based care for patients with 2+ chronic conditions. The catch: precise minutes, consent, initiating visits, 24/7 access, an electronic care plan, and strict concurrency rules.[1]
Manual Minutes = Missed Claims
Trying to hand-log 20+ minutes across dozens of micro-tasks is why many patients stall at 18 minutes and never get billed.
Common Audit Traps
Double-counted time, missing consent/initiating visit, and prohibited stacking with other services trigger denials and clawbacks.[1]
Revenue Left on the Table
Without guardrails, most programs under-bill the base 20 minutes and rarely capture lawful add-on time.
From Manual Logs to Automated, Auditable Revenue
Step 1: Automate Time Logging
FairPath captures clinical-staff time for calls, patient/caregiver communications, chart work, referrals, and care-plan updates--accumulating toward 99490/99439 or practitioner-time 99491/99437 with a defensible audit trail.[1]
Step 2: Enforce Concurrency Rules
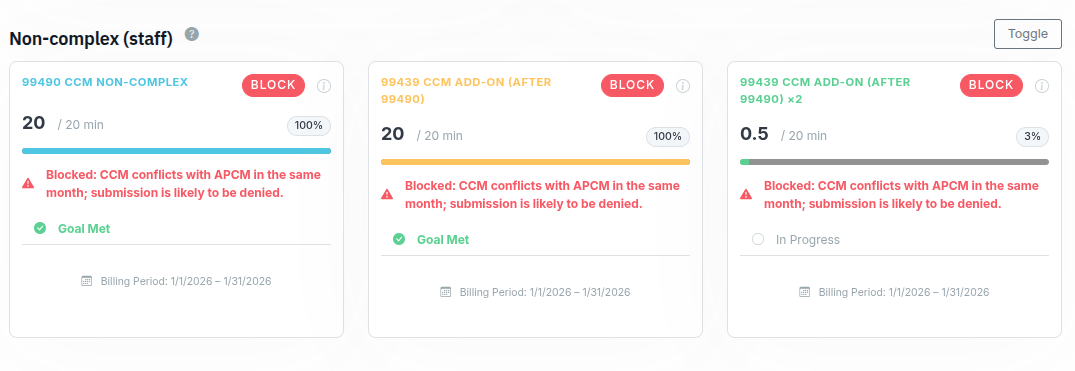
Our Compliance-as-Code engine blocks prohibited overlaps: complex vs non-complex CCM, prolonged E/M with complex CCM, and RPM or RTM (one, not both) with CCM--no double-counting minutes.[1]
Step 3: One-Click Claim Files
At month-end, FairPath surfaces patients who meet time and documentation elements (consent, initiating visit, electronic care plan, 24/7 access, transitions) and generates clean claim files.[1]
"We use the innovative templates daily to streamline our CCM care plans. It has revolutionized the care we provide and far exceeded our expectations."
Our automated care plans save clinical staff 15+ minutes per patient.
See how APOTHEcare used this to streamline workflows →
Coordinate the Whole Panel
CCM is one piece. FairPath orchestrates CCM with RPM/RTM and, when appropriate, APCM--while preventing billing conflicts.
Who Qualifies & What’s Required
Eligibility: 2+ chronic conditions expected to last ≥12 months (or until death) and posing significant risk; CCM is billed by the calendar month.[1]
Before billing: complete an initiating visit (E/M, AWV, or IPPE), obtain and document patient consent, maintain a comprehensive electronic care plan in certified EHR tech, ensure 24/7 access, and manage care transitions.[1]
Who furnishes: clinical staff may furnish CCM incident-to under general supervision; practitioner-time codes (99491/99437) require time personally by the billing practitioner.[1]
The Financials (Without the Guesswork)
Use our calculator (built on CMS PFS files) to estimate locality-specific amounts. If you prefer, look up current Medicare amounts directly in the official PFS Look-Up Tool.[3] [4]
Estimate Your CCM RevenueNote: Patient cost-sharing applies to CCM; supplemental insurance may cover coinsurance.[1]
What’s Changing in 2026?
CMS finalized APCM refinements, including optional behavioral-health add-on codes, and remote-monitoring policy updates in the CY 2026 PFS final rule. We keep our rules engine and calculator aligned with official files and MAC guidance.[5]
Your CCM Compliance Questions, Answered
Can we bill RPM and CCM in the same month?
Yes--CMS allows CCM with either RPM or RTM if each service independently meets requirements and you don’t count time twice. You cannot bill both RPM and RTM in the same month with CCM.[1]
What exactly counts toward the 20 minutes?
Care coordination and management activities like medication reconciliation, care-plan creation/revision, patient or caregiver communications, chart and lab review, referrals and follow-up, and managing transitions. Track only CCM-eligible minutes and don’t reuse those minutes for other billed codes.[1]
Who can furnish CCM and under what supervision?
Clinical staff (employees or contracted) may furnish CCM incident-to under general supervision of the billing practitioner; the practitioner provides overall direction and does not need to be physically present. Practitioner-time codes (99491/99437) require time personally by the billing practitioner.[1]
Do we need an initiating visit and consent?
Yes. For new or long-lapsed CCM patients, complete an initiating visit (E/M, AWV, or IPPE) and obtain/document patient consent (cost-sharing, that only one practitioner bills per month, and the right to stop anytime).[1]
Can we report complex CCM and regular CCM in the same month?
No. Don’t report 99487/99489 in the same calendar month as 99490/99439. Also, don’t pair practitioner-time CCM (99491/99437) with clinical-staff CCM for the same patient/month.[1]
Is CCM billed by calendar month?
Yes. CCM thresholds and codes are calendar-month based. This differs from device-supply codes in RPM/RTM, which use 30-day periods.[1]
Any special notes for RHCs/FQHCs?
RHCs/FQHCs may bill CCM and TCM for the same patient during the same period, and they follow distinct billing mechanics. Confirm current MAC guidance for your setting.[1]
References
- CMS MLN Booklet: Chronic Care Management Services (ICN MLN909188, June 2025). Includes eligibility, initiating visit & consent, electronic care plan/EHR, 24/7 access, supervision, code times, and concurrent billing rules (e.g., CCM with RPM or RTM; no double-counting). PDF
- CMS: Advanced Primary Care Management (APCM) Services overview (May 12, 2025). Monthly bundle; auxiliary personnel under general supervision; integrates CCM-like elements. Web
- CMS: PFS Look-Up Tool Overview (official rate lookup). Web
- CMS: Search the Physician Fee Schedule (interactive search). Web
- CMS Fact Sheet: CY 2026 Medicare Physician Fee Schedule Final Rule (Oct 31, 2025). APCM add-ons and related updates. Web