If your RPM, CCM, or RTM vendor is charging a percentage of collections, you may have a federal fraud-and-abuse problem that neither of you is talking about. It is the most common vendor pricing model in remote care, and it is structurally the hardest to defend under the Anti-Kickback Statute and the Stark Law.
We just published a full compliance guide on percentage-of-collections vendor compensation in RPM, CCM, and RTM that explains the legal framing, the common traps, and safer pricing alternatives. Below is a practical breakdown of what it means and what to do next.
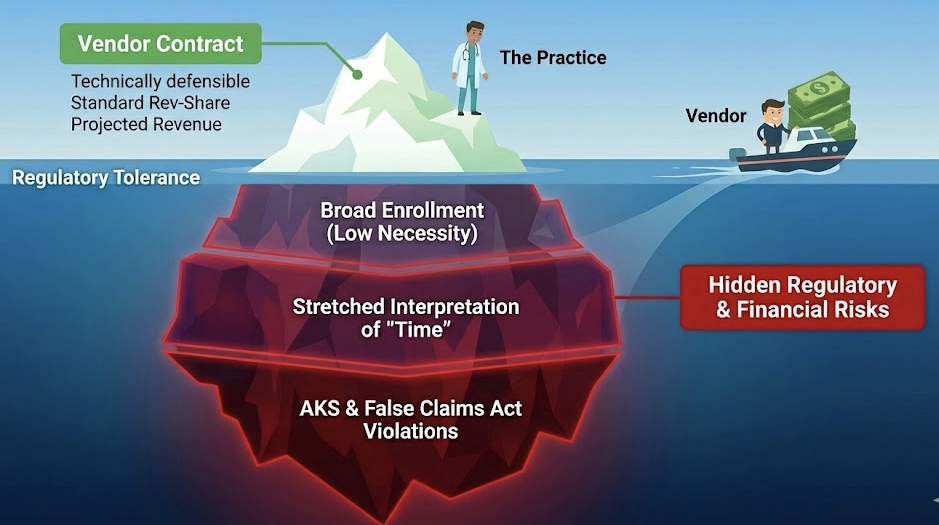
The Core Problem
A vendor fee that rises and falls with Medicare collections looks like paying for the volume or value of federally reimbursed business. That is exactly what the Anti-Kickback Statute (AKS) prohibits: remuneration intended to induce or reward referrals or orders of items/services reimbursable by a federal health care program. It is a felony statute.
Separately, the Stark Law prohibits physicians from referring Medicare patients for designated health services to an entity with which the physician has a financial relationship, unless an exception applies. A percentage-of-collections arrangement creates a financial relationship that is very difficult to fit into a safe harbor or exception.
The Question You Should Be Asking
The practical question is not "is revenue share always illegal?" The real question is: does the compensation method create a plausible inducement narrative or violate the conditions of the main safe harbor/exception you would need to rely on?
If your vendor contract says "15% of collections" and the vendor is involved in enrolling patients, managing devices, or producing documentation that drives billing, the answer is probably yes.
Common Traps
- Variable rate based on collections volume - the more you bill, the more the vendor earns. This is the textbook AKS trigger.
- Vendor involvement in enrollment or documentation - if the vendor is generating the evidence that supports the claim and also taking a percentage of the claim, the inducement narrative writes itself.
- No written agreement or stale agreement - AKS safe harbors and Stark exceptions require a signed, current, compliant written agreement.
- Fair market value not documented - if the percentage bears no relationship to the actual cost of services rendered, you cannot defend it as fair market value.
Safer Alternatives
The guide covers fixed-fee-per-patient, per-month pricing, cost-plus models, and flat-rate service agreements that are much easier to defend. The key principle: the vendor's compensation should not vary based on the volume or value of Medicare business you generate.
The Bottom Line
If you are in a percentage-of-collections arrangement, you do not need to panic, but you do need to review the contract with counsel and understand your exposure. The safest path is to renegotiate to a fixed-fee structure before the OIG or a whistleblower comes looking.
The full guide with legal framing, trap analysis, and safer pricing models is at Percentage-of-Collections Vendor Compensation in RPM, CCM, and RTM.
Related resources: Converting CPAs into Revenue Contracts Without Stark or Anti-Kickback Exposure, Vendor Exit Blueprint, The OIG's 2026 RPM Audit is Scheduled: Are You Ready?.
Disclaimer: This article is informational only and is not legal advice. Coverage, coding, and rates vary by Medicare Administrative Contractor (MAC) and payer plan. Review vendor contracts with qualified counsel.