Percentage-of-Collections Vendor Compensation in RPM, CCM, and RTM
Why revenue share creates AKS and Stark risk (Updated 2026)
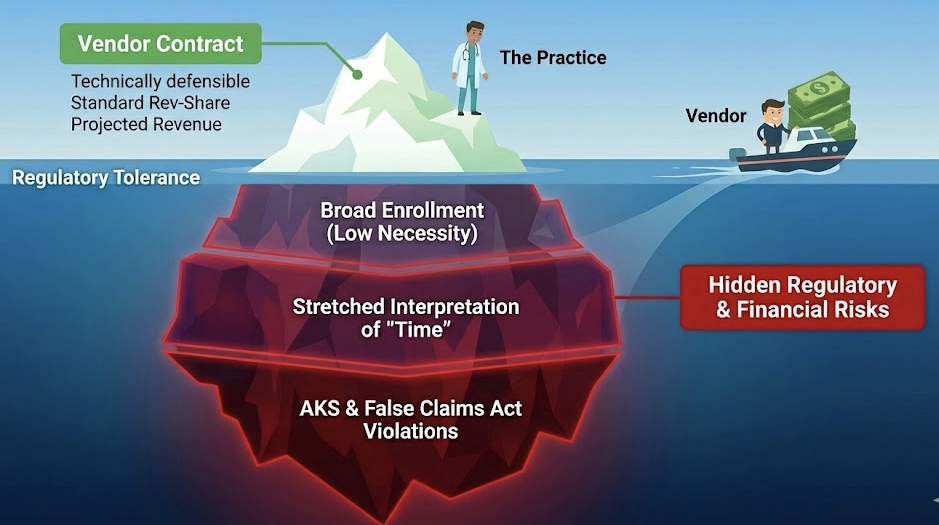
A vendor fee that rises and falls with RPM/CCM/RTM collections is structurally hard to defend under federal fraud-and-abuse rules because it looks like paying for volume/value of federally reimbursed business.
Compliance note: This page is informational and operational. It is not legal advice and does not replace counsel.
Overview
Practices often want vendor pricing that “scales with revenue.” Vendors often want a share of collections because it reduces their sales friction and shifts downside risk to the practice.
Federal fraud-and-abuse laws push in the opposite direction: they are designed to prevent financial incentives from distorting medical decision-making and utilization. The Anti-Kickback Statute (AKS) makes it a felony to pay or receive remuneration to induce or reward referrals or orders of items/services reimbursable by a federal health care program. (law.cornell.edu)
Separately, the Stark Law prohibits physicians from referring Medicare patients for designated health services (DHS) to an entity with which the physician has a financial relationship, unless an exception applies, and it prohibits billing for DHS furnished pursuant to a prohibited referral. (law.cornell.edu)
Your practical question isn’t “is revenue share always illegal?” The real question is: does the compensation method create a plausible inducement narrative or violate the conditions of the main safe harbor/exception you’d need to rely on?
Key Takeaway in One Sentence
Core Rule Explanation
1) Anti-Kickback Statute: the baseline prohibition
AKS covers paying or receiving “remuneration” to induce or reward referrals or ordering/arranging/recommending items or services payable by a federal health care program. The statute is written broadly and explicitly reaches payment intended to induce referrals or induce purchasing/ordering/arranging/recommending. (law.cornell.edu)
2) The safe harbor most people point to: 42 C.F.R. § 1001.952(d)
The personal services and management contracts safe harbor (as updated) requires, among other things, a written agreement, at least a 1-year term, and critically:
- The methodology for determining the compensation must be set in advance and must not take into account the volume or value of referrals or business otherwise generated between the parties for which payment may be made by federal programs. (law.cornell.edu)
OIG’s 2020 rulemaking explicitly replaced the older “aggregate compensation set in advance” requirement with “methodology set in advance,” but it emphasized that safe harbor protection still does not extend to arrangements where aggregate compensation is determined in a manner that takes into account volume/value of referrals or business generated. (Federal Register)
3) Stark Law: when it matters here
Stark applies when a physician is referring for designated health services (DHS) to an entity with which there’s a financial relationship and no exception, and it prohibits billing for DHS furnished pursuant to a prohibited referral. (law.cornell.edu)
If Stark is implicated (fact-dependent), common compensation exceptions require compensation set in advance, FMV, and not determined in a manner that takes into account the volume or value of referrals or other business generated. (law.cornell.edu)
Common Failure Patterns / Traps
Trap 1: “It’s not a referral fee, it’s just how we price the service”
In practice, a revenue share behaves like a referral- or volume-linked fee because the vendor’s compensation rises when the practice bills more reimbursable RPM/CCM/RTM units (or collects more dollars per unit).
Trap 2: Bundling “marketing/enrollment” into the vendor scope while paying a percent of collections
OIG has warned practitioners to use heightened scrutiny when entering arrangements with telemedicine companies that include suspect characteristics such as patients being recruited by marketing channels and practitioners being paid based on the volume of items or services ordered/prescribed. (Office of Inspector General)
Trap 3: “We’ll carve out Medicare and keep the percentage for commercial only”
OIG has been explicit that percentage compensation is “inherently problematic,” and it has also warned that “carve outs” and non-federal funding sources are not dispositive for AKS intent analysis. (Office of Inspector General)
Trap 4: “We don’t pay for referrals; we pay for billing”
OIG has long flagged that percentage-based billing arrangements can create incentives to maximize revenue and increase abusive billing risk, and has described management companies being paid a percentage of net revenues as potentially prohibited remuneration in specific fact patterns. (Office of Inspector General)
Why This Is Non-Compliant
1) Safe harbor mismatch: the methodology is volume/value-linked
A classic “vendor gets X% of collections for RPM/CCM/RTM” is hard to reconcile with the safe harbor condition that the compensation methodology must not take into account the volume or value of referrals/business generated. (law.cornell.edu)
2) OIG’s repeated posture: percentage compensation is “inherently problematic”
OIG has stated directly that “percentage compensation arrangements are inherently problematic” because they relate to the volume and value of business generated between parties. (Office of Inspector General)
3) The 2024–2025 RPM oversight environment makes “incentives” look worse, faster
OIG’s 2024 report found that about 43% of RPM enrollees did not have claims/encounter records for all three RPM components and stated Medicare lacked key oversight information such as ordering provider data. (Office of Inspector General)
OIG’s 2025 RPM report reported $536 million in RPM payments in 2024 (31% increase from 2023) and described monitoring measures such as billing RPM for patients with no prior relationship and billing multiple monitoring devices per enrollee per month. (Office of Inspector General)
4) Marketing/referral payments are actively enforced in RPM-adjacent contexts
DOJ publicly announced a 2025 settlement involving an RPM company alleged to have violated AKS/FCA by paying a marketing service for referrals of Medicare beneficiaries. (Department of Justice)
Edge Cases & Clarifications
Does failing a safe harbor automatically mean the deal is illegal?
No. Safe harbors are voluntary and failing to fit one does not make an arrangement per se unlawful; the analysis becomes facts-and-circumstances. (Office of Inspector General)
What if the vendor only provides software and we do everything else?
That reduces some risk drivers (marketing, ordering influence, patient steering), but it doesn’t fix the core issue: the vendor is still paid by a formula keyed to federally reimbursed dollars.
Does Stark apply to RPM/CCM/RTM vendor fees?
Sometimes; often not directly. Stark becomes more relevant when DHS is involved and the entity receiving referrals/billing DHS is the one with the financial relationship. Regardless, Stark’s common exceptions also contain “set in advance” and “no volume/value” conditions that conflict with percentage-based formulas. (law.cornell.edu)
State law note: Even if a structure survives federal analysis, state fee-splitting, corporate practice of medicine, and state anti-kickback analogs can independently prohibit percentage-based arrangements. Treat state law as a separate gating step.
Forward-Looking Policy Changes
What is clearly “moving” (without speculating about future rule text) is oversight intensity:
- OIG’s 2024 RPM report includes recommendations with future expected updates and explicitly calls for identifying and monitoring companies billing RPM. (Office of Inspector General)
- OIG’s 2025 report adds concrete monitoring measures and frames them as tools to identify practices that “warrant further scrutiny.” (Office of Inspector General)
Practically: incentive-aligned billing growth models are becoming less tolerable in an environment that is instrumenting “billing anomaly detection” for RPM.
Practical Implications for Practices
Stop doing
Signing new RPM/CCM/RTM vendor contracts where payment is a percentage of collections, receipts, or revenue attributable to federally reimbursed services, without a hard, defensible rationale and counsel review.
Change to
Reframe vendor pricing around service units and FMV (PPPM for active managed patients, flat platform fee, fixed hourly for defined labor) rather than reimbursed dollars collected.
Planning Checklist
- Inventory every vendor arrangement touching RPM/CCM/RTM and label the compensation type (percent-of-collections, per-patient, flat fee, hourly).
- Identify whether the vendor (or anyone downstream) performs or funds marketing, patient recruitment, call-center outreach, enrollment, or ordering facilitation.
- If any contract is percentage-based: document why the methodology does not take into account volume/value of federal program business, document FMV/commercial reasonableness, and require counsel review before renewal.
- Prefer re-papering to fixed PPPM (defined “active management” criteria), flat monthly/annual platform fee tied to scope, or fixed hourly for delineated staff functions with timekeeping.
- Ensure the contract explicitly defines scope, term (≥ 1 year), and the compensation methodology up front.
- Build audit-ready evidence: what services were delivered, by whom, when, and how medical necessity and ordering responsibility are established.
How FairPath Automates or Enforces This
Reading the law is one thing. Enforcing it across thousands of patients, multiple vendors, and changing payer behavior is another.
FairPath’s approach is to encode “compensation risk logic” and “program integrity signals” as operational controls:
- Contract structure linting: flag percentage-of-collections language and require an explicit compliance rationale before a contract can be marked “approved for Medicare-facing workflows.”
- Scope-to-compensation consistency checks: if a vendor scope includes enrollment/marketing-like activities, automatically elevate the risk rating and require additional controls.
- Evidence-first audit trails: store the who/what/when evidence needed to support the underlying service.
- Billing-pattern monitoring: mirror OIG-style anomaly patterns (spikes, lack of prior relationship, multiple devices) as internal alerts.
FAQ
References
- Anti-Kickback Statute (42 U.S.C. § 1320a-7b(b)) (law.cornell.edu)
- AKS safe harbor: 42 C.F.R. § 1001.952(d) (law.cornell.edu)
- OIG Final Rule (Dec 2, 2020) (Federal Register)
- OIG Advisory Opinion 98-04 (Office of Inspector General)
- OIG Advisory Opinion 06-02 (Office of Inspector General)
- Stark Law (42 U.S.C. § 1395nn) (law.cornell.edu)
- Stark compensation exception language (42 C.F.R. § 411.357) (law.cornell.edu)
- OIG Report: Additional Oversight of RPM in Medicare Is Needed (Sep 19, 2024) (Office of Inspector General)
- OIG Report: Billing for RPM in Medicare (Aug 25, 2025) (Office of Inspector General)
- OIG Special Fraud Alert: Telemedicine/telehealth suspect characteristics (July 20, 2022) (Office of Inspector General)
- OIG Special Fraud Alert: Suspect payments in MA marketing arrangements (Dec 11, 2024) (Office of Inspector General)
- DOJ Press Release: LiveCare RPM settlement (Jan 31, 2025) (Department of Justice)
FairPath is designed to handle this complexity for you.
While most platforms simply record what happened, FairPath actively runs the program. It continuously monitors every patient, staff action, and billing rule across CCM, RPM, RTM, and APCM, intervening immediately when a requirement is missed.
This allows you to scale your own program without losing quality, breaking trust with physicians, or losing control of your revenue. We provide the precision of an automated medical director without the chaos.