APCM Eligibility, Attribution, and Continuity: Why CMS Now Treats Them as One System
CMS has fused APCM eligibility, practitioner attribution, and continuity into a single monthly operating system--billing without that coherence now creates denial and audit exposure.
This is an operational guide grounded in public CMS materials--not legal advice. Confirm billing decisions with your MAC and current CMS guidance.
CMS 2026 Signal
Eligibility, attribution, and continuity must reconcile inside the same billing month--CMS is paying for longitudinal ownership, not isolated events.
Billing APCM without month-specific attribution integrity, an active care plan, and continuity evidence bakes denials and audit exposure into your model.
Overview
APCM is Medicare’s monthly payment model for longitudinal, team-based primary care. It is built around continuity, access, care planning, coordination, and population-level management as part of ongoing responsibility for a panel. ([CMS][1])
CMS’s 2026 moves make the “one system” point concrete:
- Behavioral-health add-ons (G0568, G0569, G0570) must be billed in the same month and by the same practitioner who bills APCM, embedding integrated BH inside primary care ownership. ([CMS][2])
- Shared Savings Program assignment now counts APCM + BHI/CoCM add-ons as primary-care services for beneficiary assignment, tying APCM/BH activity directly to attribution and quality mechanics. ([CMS][3])
Result: eligibility, attribution, and continuity cannot be separated operationally--they must reconcile inside each billing month.
Section Index
- Key Takeaway in One Sentence
- What “Eligibility” Really Means Under APCM
- Attribution Is Responsibility, Not Enrollment
- Continuity as a Billing Primitive
- The Care Plan: The Minimum Viable Continuity Artifact
- Common Failure Patterns
- Why These Patterns Fail an Audit
- Edge Cases & Clarifications
- Forward-Looking CMS Direction
- Practical Implications for Practices
- Planning Checklist
- How This Fits the Bigger CMS Story
- How FairPath Automates and Enforces This
- FAQs
- References
1. Key Takeaway in One Sentence
APCM billing is defensible only when eligibility, practitioner attribution, and continuity evidence reconcile within the same billing month--because CMS is explicitly aligning APCM payment, behavioral add-ons, and assignment logic around longitudinal primary care ownership. ([CMS][1])
2. What “Eligibility” Really Means Under APCM
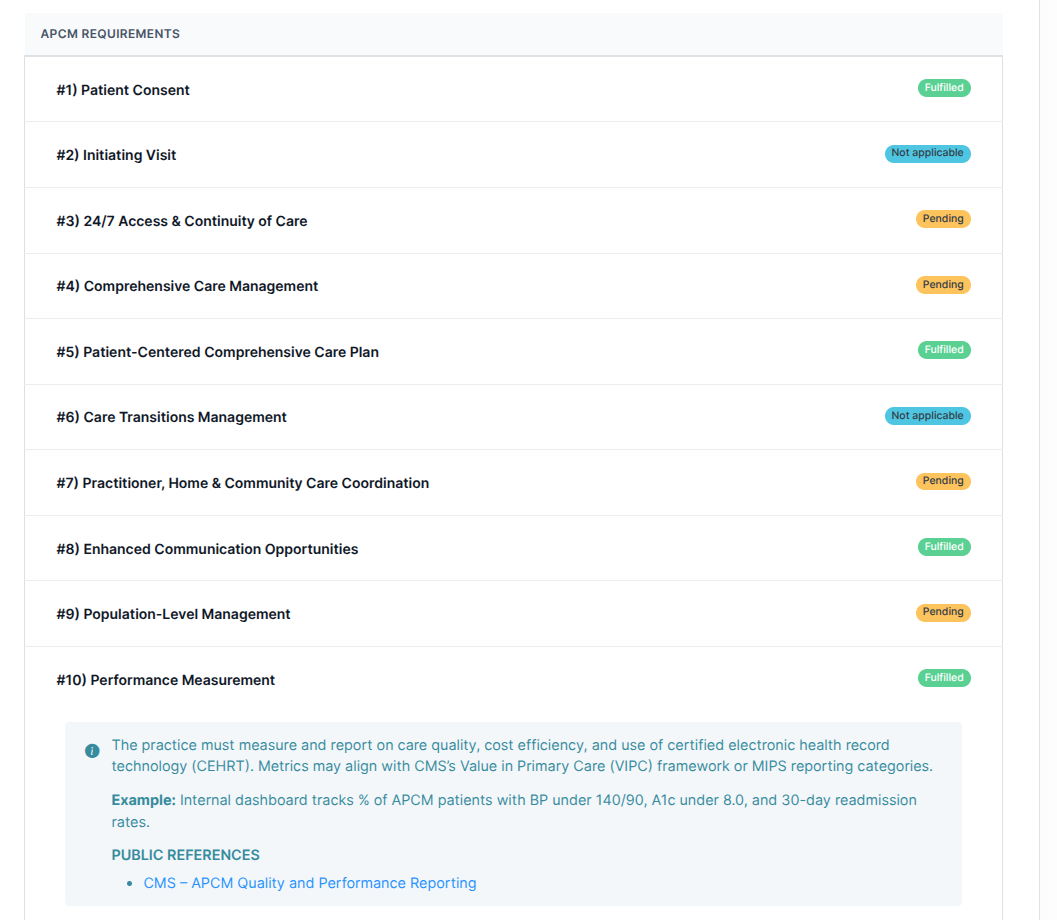
APCM is not a static enrollment flag. CMS frames APCM as a monthly service with defined requirements: consent, initiating visit logic (with exceptions), 24/7 access and continuity expectations, a comprehensive care plan, care transitions, coordination, enhanced communication, population-level management, and performance measurement. ([CMS][1])
- Eligibility is month-specific. You furnish APCM only when the practice is operating the APCM model for that patient this month.
- Eligibility is contextual. If you cannot show longitudinal management this month, you are depending on a story an auditor is not obligated to accept.
3. Attribution Is Responsibility, Not Enrollment
Attribution answers which clinician/team is accountable for ongoing primary care management. CMS now counts APCM + BHI/CoCM add-ons as primary-care services for SSP beneficiary assignment, making attribution a payment and quality construct rather than a marketing roster. ([CMS][3])
- Patients can stay attributed without documented longitudinal management.
- Staff can work without anchoring to the attributed practitioner’s plan-of-care and monthly review.
- BH activities can drift away from the same-month/same-practitioner rule.
4. Continuity as a Billing Primitive
Continuity is baked into APCM requirements: the ability to schedule successive routine appointments with a designated team member, 24/7 access for urgent needs, and longitudinal management. ([CMS][1])
- You prove continuity with a monthly pattern: a living care plan, accountable clinician/team, documented coordination and follow-ups.
- A single note is not enough; the story must hold together inside the billed month.
5. The Care Plan: The Minimum Viable Continuity Artifact
CMS expects a patient-centered comprehensive care plan as part of APCM. ([CMS][4]) It is the simplest defensible continuity artifact: the longitudinal spine auditors understand.
- If you bill a longitudinal service, you need a longitudinal artifact.
- Use the care plan as the canonical place to show “this month” continuity without inventing fragile proxies.
- APCM Care-Plan Readiness % (month) = (Patients in active panel with a qualifying care-plan update dated in the current month) ÷ (Active panel size) × 100.
Low readiness means your claims assert longitudinal management that your documentation cannot prove.
6. Common Failure Patterns
1) Passive attribution
Patients stay on panels for months with minimal longitudinal documentation or care-plan maintenance.
2) “Enrollment = eligibility” drift
Consent is collected once; APCM is billed repeatedly without month-specific evidence of APCM service elements.
3) Stale longitudinal plans
Care plans exist but are treated as onboarding paperwork instead of living artifacts.
4) Fragmented services that don’t reconcile
BH integration or monitoring activity is not clearly tied to the attributed practitioner, the APCM month, or the maintained plan.
5) Same-month rule violations
BH add-ons are delegated to different clinicians or external teams, making the same practitioner/same month rule hard to satisfy. ([CMS][2])
7. Why These Patterns Fail an Audit
Audits collapse complex reality into a simple question: Does the record support what the claim asserts, in the time period billed, under the responsible clinician?
- Time-period integrity: APCM is billed this month, but evidence is stale or backfilled.
- Responsibility integrity: work exists, but attribution and practitioner responsibility are unclear.
- Claims coherence: APCM + BH add-ons and other longitudinal services do not connect logically for a reviewer.
OIG scrutiny of longitudinal billing (e.g., CCM overpayments; RPM oversight signals) shows enforcement follows expansion. ([Office of Inspector General][5])
8. Edge Cases & Clarifications
“Nothing changed clinically this month--do we still need to update the plan?”
You need month-specific evidence of review/management. A lightweight “reviewed and remains appropriate” attestation tied to the plan preserves time-period integrity.
“Patient didn’t engage. Can we still bill APCM?”
Document outreach attempts, coordination actions, and plan review decisions. Attribution means responsibility even when the patient is quiet.
“Can RPM/RTM time serve as APCM continuity evidence?”
Only if explicitly anchored to the APCM plan-of-care and month-specific practitioner responsibility. Keep streams separate to avoid double-counting, but link monitoring artifacts to the APCM plan.
“What if attribution changes mid-month?”
Snapshot attribution for billing periods so you can show responsible clinician/team as-of the APCM month for auditability.
9. Forward-Looking CMS Direction
- APCM base requirements emphasize continuity and a maintained care plan. ([CMS][1])
- APCM BH add-ons require same-month/same-practitioner attachment. ([CMS][2])
- SSP assignment counts APCM + BHI/CoCM add-ons as primary care services. ([CMS][3])
The direction: claims-level coherence--services must hang together as a longitudinal model, not isolated billing events.
10. Practical Implications for Practices
- Stop treating APCM as a passive monthly charge attached to “enrolled” patients.
- Treat attribution as responsibility: enforce panel hygiene, manage drift, and document continuity.
- Maintain a living care plan with at least one month-specific ownership signal.
- Ensure BH and monitoring services map back to the APCM plan spine and billing practitioner accountability.
- Build pre-claim controls that block weak months before denials and audits do it for you.
11. Planning Checklist
- Audit your active attributed panel for stale care plans, missing month-specific ownership signals, and unclear responsible clinicians.
- Define what “qualifying care-plan update” means (edit, goal update, review attestation, patient acknowledgment).
- Implement a month-end APCM validator that blocks billing if continuity evidence is missing for that month.
- Train clinicians on lightweight attestation workflows to avoid note bloat while preserving defensibility.
- For BH add-ons: enforce a same practitioner/same month guardrail at charge capture. ([CMS][2])
- If you participate in SSP/ACO models: align your operational definition of “primary care services” with CMS’s updated assignment definition (including APCM + BHI/CoCM add-ons). ([CMS][3])
12. How This Fits the Bigger CMS Story
CMS is moving from reimbursing measurable tasks to reimbursing longitudinal accountability and integrating behavioral health into primary care ownership.
- Old world: isolated events and minute counts.
- New world: longitudinal ownership, integrated BH, and attribution-aware quality/payment.
- APCM is the payment structure; attribution and continuity are the enforcement substrate.
13. How FairPath Automates and Enforces This
- Eligibility is month-specific. We do not treat patients as “enrolled forever.”
- Attribution is snapshotted per billing period for auditable responsible clinicians/teams.
- Continuity is evidenced via care-plan versioning, monthly review attestations, and structured plan-impact events.
- BH add-ons are gated by same-month/same-practitioner rules at charge capture and claim generation. ([CMS][2])
- Pre-claim validation blocks APCM billing when continuity evidence is missing.
Result: claims and documentation stay coherent--eligibility, attribution, and continuity reconcile before submission.
14. FAQs
What are the APCM base requirements we must operationalize?
Consent, initiating-visit logic for new patients (with defined exceptions), 24/7 access and continuity expectations, comprehensive care management, a patient-centered care plan, care transitions, coordination, enhanced communication, population-level management, and performance measurement. ([CMS][1])
Do we need a care-plan update every month to bill APCM?
You need month-specific evidence of ongoing management. A lightweight plan review/attestation can be sufficient when no substantive edits are needed because it preserves time-period integrity.
Are the APCM behavioral-health add-ons optional?
Yes. CMS finalized optional BH add-on codes for APCM. They must be billed in the same month by the same practitioner as the APCM base code. ([CMS][2], [CMS][6])
What is the most important billing constraint for the APCM behavioral add-ons?
Same practitioner, same month as the APCM base code. They are designed to sit inside the primary care ownership model, not float independently. ([CMS][2])
Why does SSP assignment matter if we’re “just billing APCM”?
CMS is aligning the definition of primary care services for SSP assignment with PFS payment changes, including APCM + BHI/CoCM add-ons. That ties APCM+BHI/CoCM activity to attribution mechanics beyond fee-for-service billing. ([CMS][3])
Can we bill APCM if only staff (not the practitioner) did work this month?
APCM is team-based, but documentation must support practitioner accountability for longitudinal management and APCM requirements. Capture explicit review/attestation and plan-of-care responsibility in the billed month. ([CMS][1])
Does virtual direct supervision “unlock” APCM?
Virtual direct supervision clarifies how immediate availability is satisfied for services requiring direct supervision; it does not expand who can do the work or what counts. ([CMS][6])
How should we store evidence to defend APCM in an audit?
At minimum: consent record; initiating visit logic; attribution snapshot per month; care-plan versioning or monthly review attestation; evidence of access/continuity processes; and structured care-coordination events mapped to the plan.
15. References
- [1] CMS: Advanced Primary Care Management Services. CMS
- [2] CMS: MM14315 CY 2026 Final Rule Summary (behavioral-health add-on constraints). CMS
- [3] CMS: CY 2026 Medicare Physician Fee Schedule Final Rule (CMS-1832-F) Shared Savings Program changes. CMS
- [4] CMS: CY 2025 Medicare Physician Fee Schedule Final Rule (care plan expectations). CMS
- [5] HHS OIG: Medicare Continues To Make Overpayments for Chronic Care Management (program integrity precedent). Office of Inspector General
- [6] CMS: CY 2026 Medicare Physician Fee Schedule Final Rule Fact Sheet (virtual direct supervision; BH add-on context). CMS
- [7] Federal Register: CY 2026 PFS Final Rule. Federal Register
FairPath is designed to handle this complexity for you.
While most platforms simply record what happened, FairPath actively runs the program. It continuously monitors every patient, staff action, and billing rule across CCM, RPM, RTM, and APCM, intervening immediately when a requirement is missed.
This allows you to scale your own program without losing quality, breaking trust with physicians, or losing control of your revenue. We provide the precision of an automated medical director without the chaos.