How UnitedHealthcare’s 2026 Policies Change RPM
A survival guide for APCM, CCM, and Vendor Models under the new restrictions.
How to use this page: Use as a planning guide, not legal advice. Confirm coverage with your specific UHC contracts.
Policy Snapshot
- Heart Failure
- Pregnancy (HDP)
Overview
Effective January 1, 2026, UnitedHealthcare (UHC) will:
-
Treat Remote Physiologic Monitoring (RPM) as a covered service only for two conditions:
- Chronic heart failure (HF)
- Hypertensive disorders of pregnancy (HDP)
-
Consider RPM “unproven and not medically necessary” for essentially all other conditions that RPM vendors commonly target, including:
- Diabetes
- Hypertension (other than HDP)
- COPD
- Obstructive sleep apnea
- Depression, anxiety, bipolar disorder, and other behavioral conditions
UnitedHealthcare’s December 2025 Medical Policy Update Bulletins and related documents:
- Introduce RPM as a new medical policy, effective Jan 1, 2026, across multiple product lines.
- Provide detailed coverage criteria in the Surest (Bind) bulletin, which effectively sets the policy tone for UHC as a whole.
- Do not introduce new 2026 medical policies for Remote Therapeutic Monitoring (RTM), Chronic Care Management (CCM), or Advanced Primary Care Management (APCM).
This resource explains:
- Which UHC products are affected and how.
- What UHC will and will not cover under RPM in 2026.
- How this interacts with your broader APCM/CCM strategy.
- What RPM vendors and practices should do next.
Section Index
- Key takeaway in one sentence
- Where the new RPM policy lives (product by product)
- What’s not in the bulletins (RTM, CCM, APCM)
- Practical coverage rules for RPM under UHC in 2026
- The pulmonary fluid monitoring nuance (Community Plan of PA)
- Implications for RPM vendors and practices
- 2026 planning checklist for practices
- What to do next
- How this fits the bigger CMS/APCM story
- How we automate this rule
- Frequently Asked Questions
- References
1. Key Takeaway in One Sentence
From January 1, 2026, UnitedHealthcare will pay for Remote Physiologic Monitoring only in narrowly defined cases (heart failure and hypertensive disorders of pregnancy) and will treat RPM as unproven/not medically necessary for most other conditions. No new 2026 UHC medical-policy bulletins were issued for RTM, CCM, or APCM.
2. Where the New RPM Policy Lives (Product by Product)
2.1 UHC Commercial, Oxford, UMR, Individual Exchange, Medicare Advantage
In the December 2025 Medical Policy Update Bulletins, UHC lists:
-
“Remote Physiologic Monitoring (RPM)” as a New medical policy, effective Jan 1, 2026 for:
- UnitedHealthcare Commercial
- Oxford
- UMR
- Individual Exchange
- Medicare Advantage
The “quick view” summaries in these bulletins:
- Mark RPM as “New” with the January 1, 2026 effective date.
- Do not spell out the coverage criteria in the summary table itself.
However, the full Commercial policy text is consistent with the Surest bulletin: RPM is medically necessary only for HF and HDP; all other uses are considered unproven and not medically necessary.
2.2 Surest (Bind): The Clearest Statement of Coverage
The Surest Medical Policy Update Bulletin (October 2025) provides the most detailed view:
- Policy: Remote Physiologic Monitoring (RPM)
- Effective date: Jan 1, 2026
Coverage rationale:
-
Proven and medically necessary for:
- Heart failure
- Hypertensive disorders of pregnancy
-
Unproven and not medically necessary for other conditions, explicitly including:
- Anxiety
- Bipolar disorder
- Chronic obstructive pulmonary disease (COPD)
- Depression
- Diabetes mellitus (including gestational diabetes)
- Hypertension other than hypertensive disorders of pregnancy
- Obstructive sleep apnea (OSA)
- Schizoaffective disorder
The Commercial full bulletin replicates this rationale, and UHC/industry commentary confirm it applies broadly across UHC product lines.
2.3 UHC Community Plan (Medicaid)
The general Community Plan Medical Policy Update Bulletin:
- Lists Remote Physiologic Monitoring (RPM) as a New medical policy, effective Jan 1, 2026, but does not provide coverage details in the summary.
State-specific bulletins:
- Ohio: The Ohio Community Plan bulletin reviewed did not contain RPM-related changes; it focused on other services.
- Pennsylvania: Includes a separate update on an external continuous pulmonary fluid monitoring system (covered below) but no different RPM policy for HF/HDP vs other conditions.
While each state Medicaid plan has its own nuances, the broader messaging and published policies strongly indicate UHC’s Medicaid RPM coverage will track the HF/HDP limitation.
2.4 UHC West Benefit Interpretation
The West Benefit Interpretation bulletin:
- Contains no explicit RPM entries; it focuses on state-mandated benefits and DME rules.
- RPM is being addressed through the medical policy channel, not the benefit interpretation, so West markets are expected to align with the core RPM policy.
3. What’s Not in These Bulletins (RTM, CCM, APCM)
Across the December 2025 UHC bulletins:
- Remote Therapeutic Monitoring (RTM) is not discussed.
- Chronic Care Management (CCM) is not updated via these specific bulletins.
- Advanced Primary Care Management (APCM) is not mentioned.
This does not mean:
- RTM, CCM, or APCM are discontinued; it simply means no new 2026 medical-policy bulletins were issued for them in this batch. They may be governed by separate reimbursement policies, existing medical policies, or program-specific guidance.
For your planning purposes:
- RPM is the main 2026 “headline” for UHC.
- RTM/CCM/APCM remain as-is until/unless UHC publishes separate updates.
4. Practical Coverage Rules for RPM Under UHC in 2026
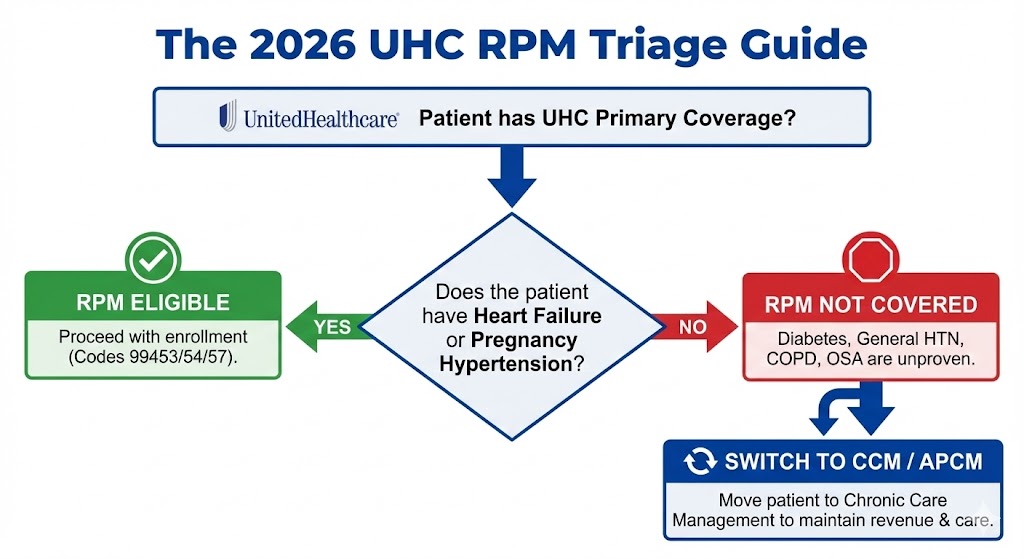
If your practice or vendor bills UHC for RPM in 2026, think in terms of “clear yes” and “clear no.”
Clear Yes (Covered)
- Chronic Heart Failure (HF)
- Hypertensive Disorders of Pregnancy
Clear No (Unproven)
- General Hypertension
- Type 2 Diabetes
- COPD / Asthma
4.1 “Clear Yes” – RPM for Heart Failure and HDP
RPM is covered, proven, and medically necessary when:
- The patient has chronic heart failure (HF), or
- The patient has a hypertensive disorder of pregnancy (HDP),
And when the clinical and documentation requirements of the policy are met (device, monitoring period, management, etc.).
4.2 “Clear No” – RPM for Most Other Chronic Conditions
RPM is explicitly unproven/not medically necessary for indications including, but not limited to:
- General hypertension (HTN) not classified as HDP
- Type 2 diabetes and gestational diabetes
- COPD
- OSA
- Depression, anxiety, bipolar disorder, schizoaffective disorder
- Other non-HF/non-HDP chronic conditions
Even if RPM has been reimbursed under UHC in the past for these conditions, the 2026 policy change draws a bright line: future RPM claims for these indications are not covered.
4.3 Devices vs RPM Professional Services
UHC has clarified in media statements that:
- It may still cover home monitoring devices (e.g., BP cuffs, glucometers) under durable medical equipment or other benefit categories,
- But it will not separately cover RPM professional service codes for most chronic conditions outside of HF and HDP.
Practically:
- Don’t confuse device coverage (a benefit question) with RPM code coverage (a medical policy question).
- You might see a BP cuff covered but RPM codes denied for a diabetic/HTN patient.
5. The Pulmonary Fluid Monitoring Nuance (Community Plan of Pennsylvania)
A separate item in the Community Plan of Pennsylvania bulletin addresses an external continuous pulmonary fluid monitoring system, where:
- The device measures pulmonary fluid levels and vital signs.
- Data is transmitted to a 24-hour attended surveillance center, then forwarded to a provider.
The 2026 update:
- Clarifies that this service is still considered unproven and not medically necessary.
- Emphasizes the definition of “remote” without changing the non-coverage status.
Important point:
- This is a distinct technology from standard RPM (e.g., home BP monitoring) and is not the same as HF/HDP RPM coverage.
- It remains off the coverage table.
6. Implications for RPM Vendors and Practices
6.1 RPM Vendors Built on UHC Revenue for Diabetes/HTN/COPD
Any RPM vendor whose business model relies heavily on:
- UHC-covered RPM visits for type 2 diabetes, non-HDP hypertension, COPD, OSA, etc.,
faces a major problem:
- UHC has effectively removed coverage for these use cases by labeling them unproven.
- Even if other payers still reimburse these indications for now, losing UHC is a significant blow in many markets.
If a vendor model is “UHC-heavy” in these categories, expect:
- Increased denials,
- Stale ROI projections,
- Tense conversations with practices who were promised “off-the-shelf RPM for everyone.”
6.2 Practices That Copied Vendor Patterns Are Exposed
If your practice:
- Has been billing UHC RPM for diabetes/HTN/COPD/OSA/etc.,
- Used vendor-defined panels and workflows,
- Relied heavily on external portals and PDFs for documentation,
then:
- Your pattern of RPM behavior is exactly the sort of thing OIG is already examining in their RPM evaluations.
- The new UHC policy doesn’t retroactively change past claims by itself, but it makes it much easier for auditors to say: “This pattern was never strongly supported, and going forward the payer will not cover it.”
The risk is especially high if:
- You cannot easily demonstrate prior relationships, medical necessity, actual device use, and real management minutes.
6.3 UHC’s Move is a “Care-First, Device-Second” Signal
UHC’s RPM stance combined with no changes to CCM/APCM in these bulletins suggests:
- UHC is willing to pay for continuous primary-care management (APCM/CCM-like constructs),
- Will only pay for RPM in limited, evidence-based conditions,
- Is not interested in funding broad device-driven RPM programs for every chronic disease.
For your strategy:
- APCM/CCM first,
- RPM second, reserved for HF and HDP (and perhaps other evidence-based cases if future policies allow).
7. 2026 Planning Checklist for Practices
Here’s a practical “pre-2026” checklist if UHC is a major payer for your panel:
- Stop launching new UHC RPM programs for diabetes, general HTN, COPD, OSA, behavioral conditions, etc.
- Segment UHC members in your RPM panel so your team does not accidentally enroll them for non-covered indications.
- Re-forecast your RPM revenue, especially if a large fraction of your diabetic/HTN patients are UHC members.
-
Audit existing HF and HDP RPM workflows:
- Confirm prior relationship, medical necessity, day counts, and management documentation.
-
Review vendor contracts:
- Identify where vendor economics assume UHC will pay for broad RPM use cases that are now disallowed.
-
Shift your remote-care roadmap toward:
- APCM/CCM for broad panel management,
- RPM only where UHC and other payers still cover it and where clinical value is clear.
-
Prepare a talking sheet for clinicians and billing:
- Clarify which conditions are “OK for UHC RPM” vs “Do not use UHC RPM codes” going forward.
8. What to Do Next
If UHC is a meaningful payer for your practice and you’re reconsidering your remote-care strategy, take control of your panel now.
Understand the Pivot
Read our full guide on CMS’ 2025–26 RPM & APCM rules and how to transition in-house.
Open the APCM/RPM GuideCheck Your Math
If you lose UHC revenue, can you afford your vendor? Run the numbers instantly.
Use the Vendor Profit AnalyzerPrepare for Audits
Worried about OIG or payer reviews? Download the 2026 Audit Survival Checklist.
Get the Audit Checklist9. How This Fits the Bigger CMS/APCM Story
UHC’s 2026 RPM changes do not exist in a vacuum. They line up with three broader trends:
- CMS is expanding APCM and other primary-care management constructs as the future of continuous care.
-
OIG has published multiple RPM evaluations showing:
- missing components (setup/device/management),
- device-only billing,
- duplicate billing and questionable patterns.
- Payors are increasingly rejecting device-driven RPM mills, especially rev-share models, and reorienting payment toward care-management and ACO-like constructs.
From FairPath’s standpoint, UHC’s RPM move is a live example of the thesis behind this product:
- Vendor-driven RPM mills were an artifact of the PHE and loose rules.
- Payers and regulators are closing that chapter.
-
The future is:
- APCM/CCM as the base,
- RPM as intensification where evidence and payers support it,
- Vendor-free, practice-owned programs where software encodes the rules and the practice owns the data, care, and revenue.
10. How We Automate This Rule
Reading the policy is one thing. Enforcing it across 2,000 patients is another. In FairPath, our Payer Ontology now reflects the 2026 UHC restrictions and automatically cross-references Payer (UHC), Diagnosis (I10 vs I50.9), and Program (RPM) so teams know where RPM is and is not covered.
- Patient records are evaluated against the updated UHC policy logic inside the Payer Ontology.
- When a UHC member is tied to a non-covered diagnosis for RPM, the enrollment workflow surfaces a clear “Not Covered” flag.
- Clinicians and staff can redirect patients into APCM/CCM-first pathways without wasting setup time or billing attempts.
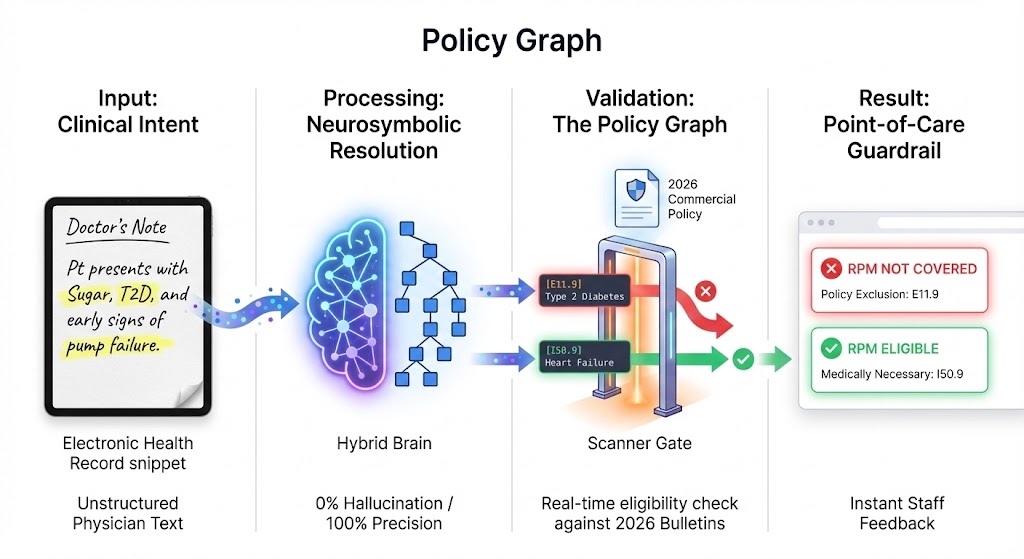
Result: you get an instant “Not Covered” flag for ineligible patients before staff time is spent enrolling them.
11. Frequently Asked Questions (FAQ)
Does UnitedHealthcare’s 2026 policy mean RPM is “dead”?
No, but under UHC it is now narrowly defined. RPM is still covered for heart failure and hypertensive disorders of pregnancy, and possibly for specific technologies under other policies. However, UHC has taken the position that RPM is unproven for many chronic conditions (like diabetes and general hypertension) that RPM vendors previously targeted.
Can we still use RPM for UHC patients with diabetes or general hypertension?
You can clinically monitor these patients however you and the patient decide, but under UHC’s 2026 medical policy, RPM professional service codes are considered unproven/not medically necessary for those indications. That means you should not expect RPM claims for these conditions to be payable under UHC.
Are home blood pressure cuffs and glucometers still covered?
In many cases, yes, as devices under members’ benefit plans or DME benefits. UHC has signaled that it may still cover home monitoring devices where appropriate. What’s changing is not the device benefit itself, but the separate RPM professional service codes for many conditions.
Does this change anything for Remote Therapeutic Monitoring (RTM)?
Based on the December 2025 bulletins, UHC did not issue new RTM medical policies for 2026. That doesn’t necessarily mean there are no RTM policies; it simply means there were no new RTM updates in this specific bulletin set. You should review UHC’s reimbursement policies and specific RTM guidance separately.
How does this impact APCM or CCM?
The December 2025 medical-policy bulletins did not introduce new APCM or CCM policies. Those services continue to be governed by existing rules and reimbursement policies. Strategically, UHC’s narrowing of RPM and the federal expansion of APCM/CCM suggest that care-management programs (APCM, CCM, BH-Collaborative Care) are where payers expect continuous care to live, with RPM as a narrower adjunct.
If we already have a vendor doing RPM for UHC diabetic and HTN patients, what should we do?
- Stop enrolling new UHC diabetic/HTN patients into RPM under the old model.
- Review the financial forecasts that vendor gave you; they’re likely no longer accurate.
- Check your contract for termination, data portability, and compliance clauses.
-
Design a transition plan where:
- You shift those patients into APCM/CCM where appropriate,
- You limit UHC RPM to HF/HDP cases,
- You consider running vendor-free, in-house remote-care programs where your team controls documentation and billing.
Is UHC’s RPM policy likely to be a trend-setter for other payers?
- limiting RPM indications,
- tying RPM more closely to documented medical necessity and continuous care programs,
- and scrutinizing rev-share vendor arrangements.
You should plan your RPM/APCM strategy so it’s resilient across payers, not designed only for one.
How should we adjust our RPM/APCM strategy if UHC is a major payer?
For UHC in particular, RPM should move from being a broad chronic-disease tool to a narrow intervention for heart failure and hypertensive disorders of pregnancy. For the rest of your chronic Medicare and commercial population, consider an APCM/CCM-first model: treat APCM (or equivalent care-management constructs) as the base for continuous care, and use RPM only where payers still cover it and where real-time data changes management. That approach is more aligned with CMS’s direction and more resilient if other payers follow UHC’s lead.
12. References
Below is a non-exhaustive list of primary and secondary sources used to build this summary. You should consult these directly before making policy decisions.
-
UnitedHealthcare Medical Policy Update Bulletins – December 2025
- UHC Commercial Medical Policy Update Bulletin (Dec 2025)
- UHC Oxford Medical Policy Update Bulletin (Dec 2025)
- UHC UMR Medical Policy Update Bulletin (Dec 2025)
- UHC Individual Exchange Medical Policy Update Bulletin (Dec 2025)
- UHC Medicare Advantage Medical Policy Update Bulletin (Dec 2025)
(All list “Remote Physiologic Monitoring (RPM)” as a new medical policy effective Jan 1, 2026.)
-
Surest (Bind) Medical Policy Update Bulletin – October 2025
- “Remote Physiologic Monitoring (RPM)” – Defines RPM as medically necessary only for heart failure and hypertensive disorders of pregnancy; deems RPM unproven/not medically necessary for multiple other conditions (anxiety, COPD, depression, diabetes, HTN, OSA, etc.).
-
UnitedHealthcare Community Plan Medical Policy Update Bulletins – December 2025
- General Community Plan bulletin announcing RPM as a new policy effective Jan 1, 2026.
- Community Plan of Pennsylvania bulletin clarifying that remote continuous pulmonary fluid monitoring (24-hour attended surveillance) remains unproven/not medically necessary.
-
UnitedHealthcare West Benefit Interpretation Policy Bulletin – December 2025
- No direct RPM entries; addresses other benefit interpretations.
-
Industry Commentary / Legal Analyses
- American Academy of Sleep Medicine (AASM) and other clinical societies’ summaries of UHC’s RPM decision.
- Law firm analyses and healthcare news reports discussing UHC’s limitation of RPM to HF and HDP and its impact on RPM vendors and practices.
FairPath is designed to handle this complexity for you.
While most platforms simply record what happened, FairPath actively runs the program. It continuously monitors every patient, staff action, and billing rule across CCM, RPM, RTM, and APCM, intervening immediately when a requirement is missed.
This allows you to scale your own program without losing quality, breaking trust with physicians, or losing control of your revenue. We provide the precision of an automated medical director without the chaos.