Stop Losing 50–70% of Remote Patient Monitoring Revenue.
Revenue-share vendors drain your margin while you hold 100% of the audit and legal liability. FairPath is the compliance-first operating system that lets your practice run RPM, APCM, RTM, and CCM on a single spine.
Updated with the latest codes and guidance for 2026 for RPM/RTM/APCM/CCM.
Who this is for
- Practices using an RPM vendor and losing margin to revenue share.
- Teams studying RPM, APCM, RTM, and CCM options.
- Leaders making remote care a stable revenue layer, not a speculative bolt‑on.
"If you want remote care to behave like part of your core practice--not a side hustle--you’re in the right place."
Vendor vs. In-House
See exactly how much revenue you lose to vendor fees vs. FairPath's flat pricing.
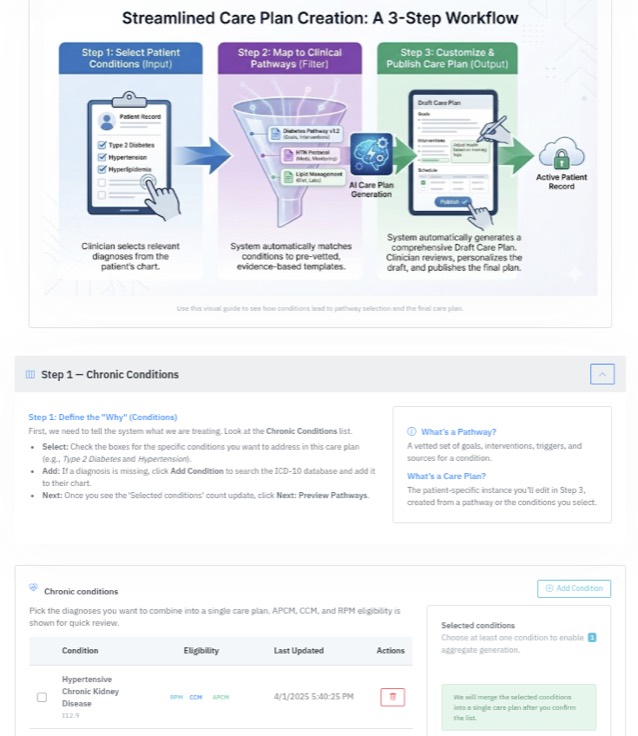
Program Design
What a Healthy Remote Patient Monitoring (RPM) Program Looks Like in 2026
Before you think about vendors, rev-share, software, or staffing, it helps to define what “good” looks like. In 2026, healthy RPM programs are targeted, layered on top of broader management models like APCM and CCM, and measured by outcomes and workload--not just codes.
Structured Patient Selection
RPM is not simply “for everyone with hypertension.” Robust programs start with a structured qualification process:
- Clinical need: diagnoses, risk, and potential benefit from monitoring.
- Payer behavior: who actually reimburses based on your own history.
- Fit with APCM/CCM: who belongs in comprehensive management instead.
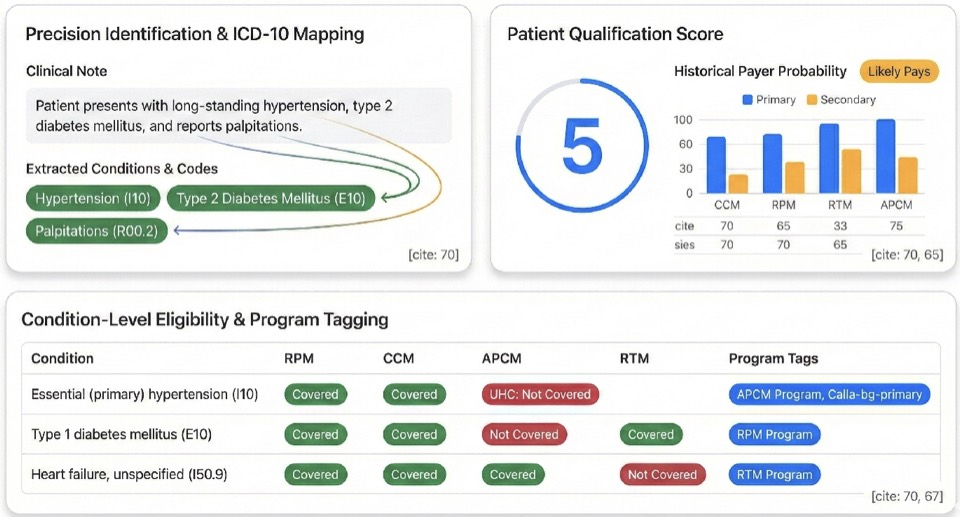
FairPath’s 1–5 Eligibility Score is one example: it consolidates diagnosis, utilization, and payment patterns into a simple, panel‑wide view of who truly fits RPM, APCM, CCM, or some combination.
RPM as a Layer, Not the Foundation
The most stable clinics treat RPM as a layer on top of a broader remote‑care spine:
- APCM (and/or CCM) as the structural base: predictable, panel‑based primary‑care management.
- RPM/RTM layered on top for patients who genuinely benefit from continuous monitoring or therapeutic tracking.
RPM‑only strategies are fragile. RPM on top of APCM/CCM is resilient and better aligned with where payers and regulators are going.
Outcomes & Workload, Not Just Codes
Healthy programs optimize for:
- Keeping high‑risk vitals in range.
- Improving adherence and self‑management.
- Supporting behavior change at scale.
And they do this while minimizing manual tracking and multiple portals, keeping staff focused on clinically meaningful work instead of “threshold management.”
FairPath was built to embody these principles: structured eligibility scoring, an APCM‑first design with RPM/RTM/CCM layered on top, and queues that direct your team to the few tasks that matter rather than chasing raw code volume.
Manage 100 or 10,000 Patients with the Same Team
One operating system for APCM, RPM, CCM, and RTM, from eligibility and onboarding to billing, compliance, and scale.
The most common objection to bringing RPM, APCM, RTM, or CCM in-house is bandwidth. FairPath’s queue-based architecture lets you work as little or as much as you want: whether you have 30 minutes a day or a dedicated team, the system prioritizes work so you never waste time, eliminate repetitive manual steps, and keep the focus on patient health first.
Eligibility & Panel Design: Stop Guessing, Start Targeting
Most practices struggle with remote care because they improvise who to enroll. FairPath replaces guesswork with structured, scalable decision-making. We turn the chaos of payer rules, diagnosis codes, and payment history into a single Qualification Score from 1 to 5 for each patient, so you see exactly who is viable for APCM, RPM, CCM, or RTM without manual chart review.
ERA & Payment Intelligence
Predictive payer scoring built from your own data. FairPath ingests your 835 (ERA) payment files to learn from your actual claims history, predicting which payers and codes will reimburse and filtering out high-denial plans before you ever start enrollment.
Condition-Level Mapping
One dashboard maps diagnoses to programs (e.g., HTN, Diabetes, COPD, CKD → APCM, RPM, CCM), showing which chronic conditions qualify for which programs in a single, simple table tuned to your clinical policies.
Always-Current Rules Engine
We automatically update the logic for CMS rules, insurance policy shifts, and ICD code changes (including ICD-11). Your eligibility scores and panel design never go stale as regulations evolve.
The Operational Shift: You never waste time chasing ineligible patients. Every enrollment minute is directed at a clinically appropriate, reimbursable candidate.
Structured Enrollment & Logistics
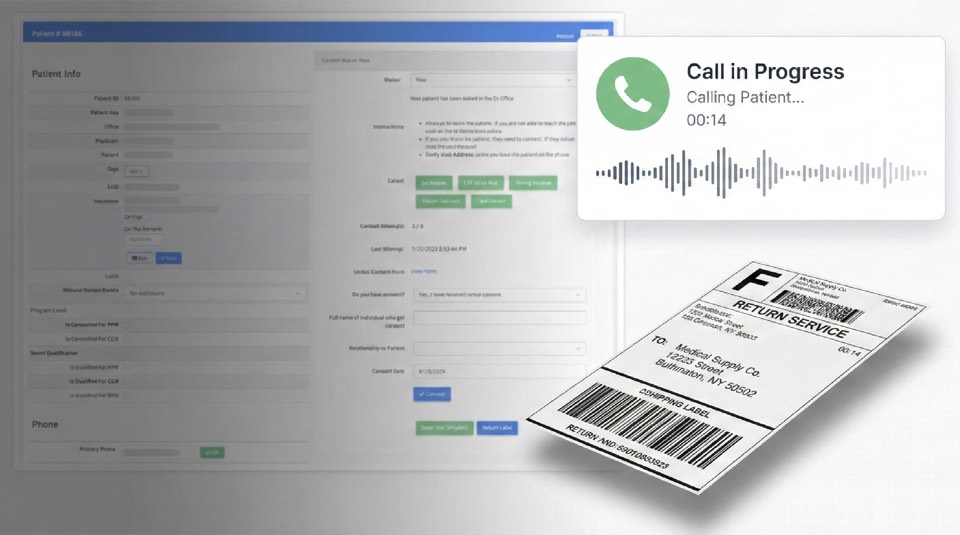
Move from “ad-hoc notes” to a structured, browser-based Onboarding Module. FairPath unifies communication, documentation, and hardware logistics in a single flow. Staff call patients from the browser, capture verbal consent, and assign device serial numbers without spreadsheets.
Call patients directly from the browser using built-in onboarding scripts. FairPath delivers training materials and automatically records and transcribes verbal consent to the chart while simultaneously kicking off downstream logistics.
Track serial numbers and assignments in one place with no separate trackers. Generate return shipping labels instantly and prevent billing for inactive or lost devices.
Send templated patient letters, save signed forms, and archive all training records in a single, audit-ready profile.
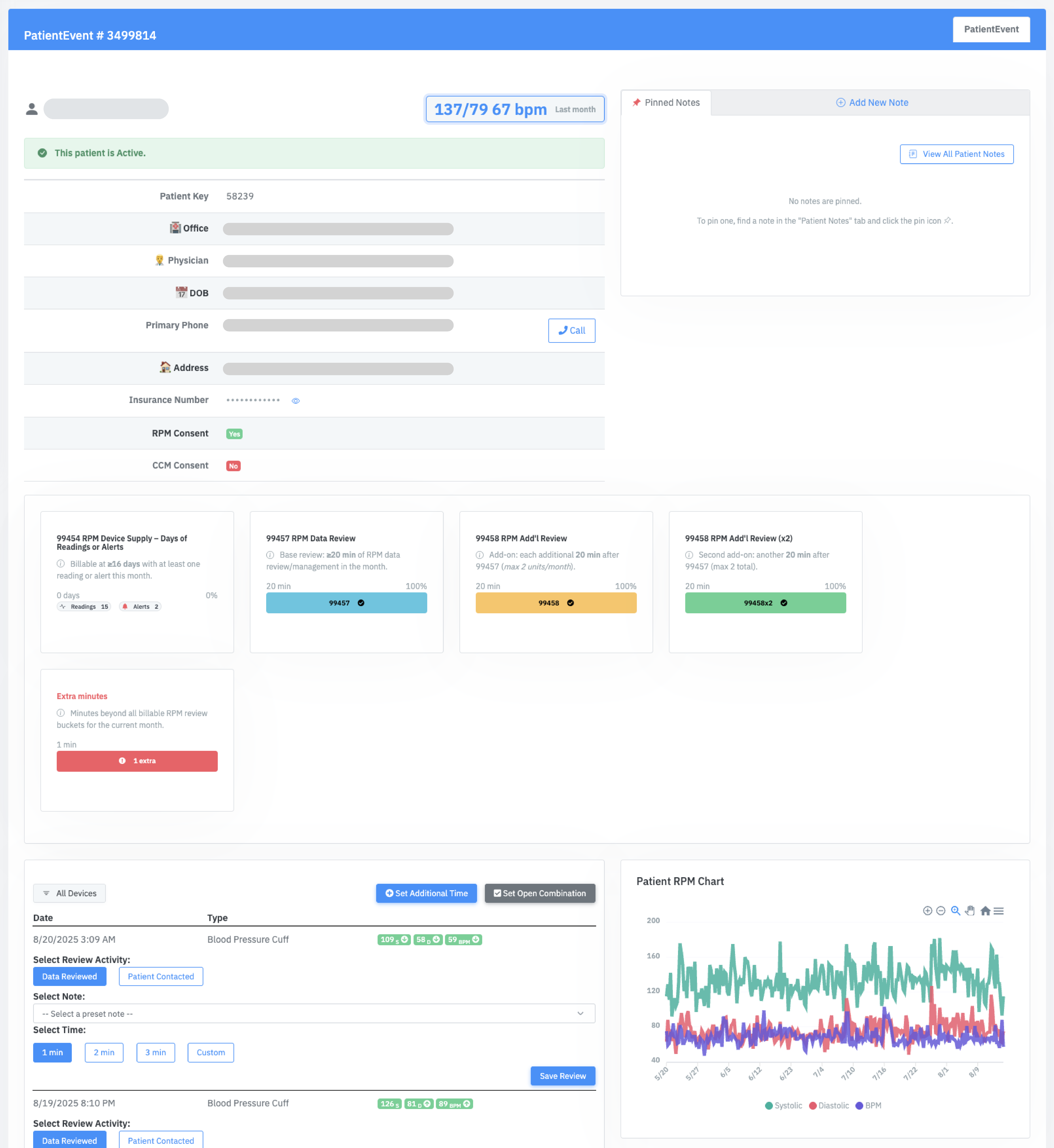
Daily Operational Command Center
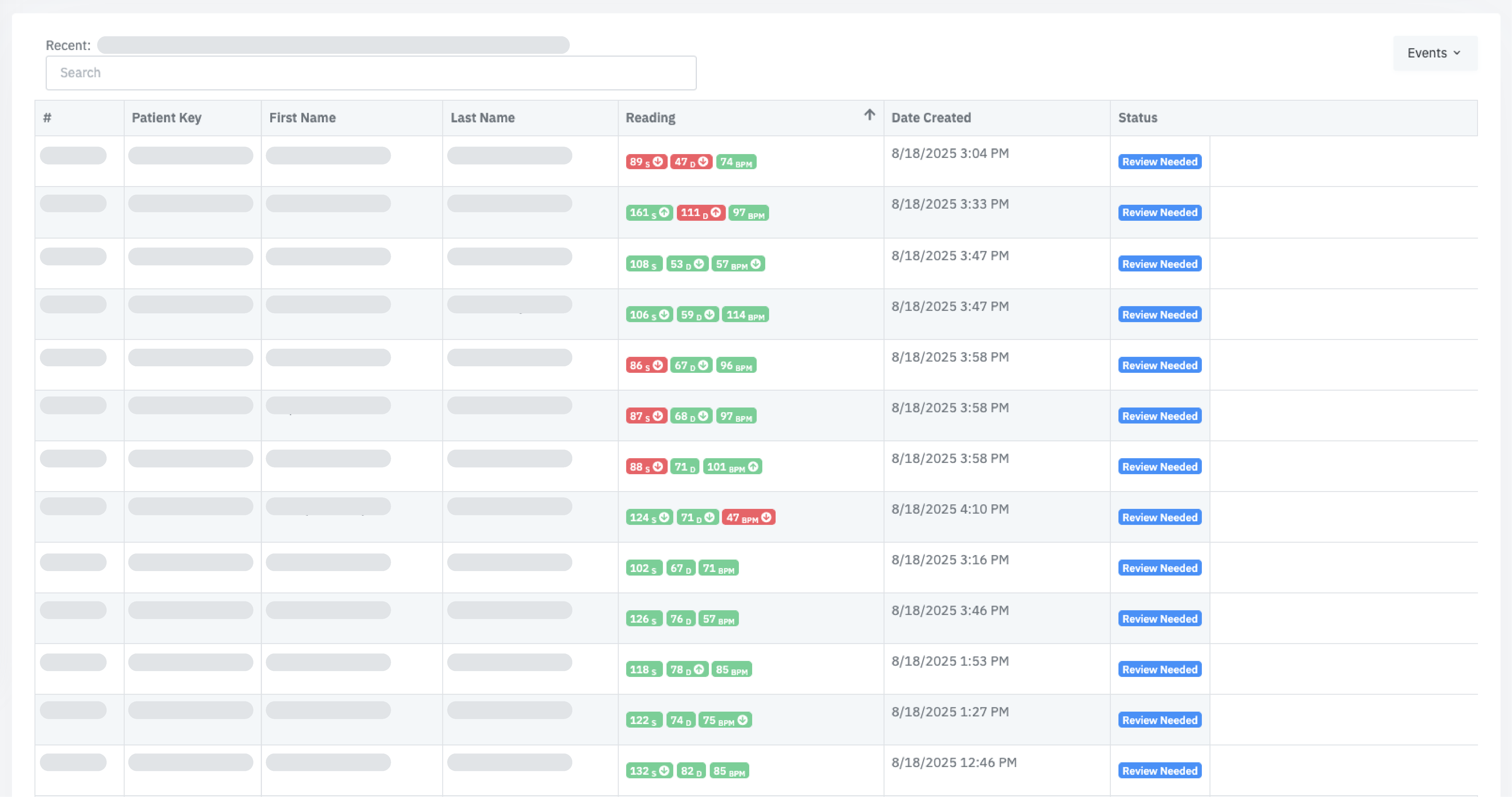
Your operations team lives in PriorityQ and ReviewQ, consolidated queues that sort work by urgency, clinical risk, and code completion. Instead of reviewing every reading, your staff works from a single queue of exceptions: critical vitals, worsening trends, and “no data” patterns. The same interface works for 50 or 5,000 patients; only the queue length changes, with Amy (AI) handling routine nudges and troubleshooting in the background.
Consolidates new readings, APCM service tasks, “Device Problem” events, and exception alerts into one prioritized list so every click advances both patient outcomes and billing progress.
Calls and texts are initiated from the queue. Every interaction is timestamped and attached to the patient record, feeding BillingQ and your audit trail automatically.
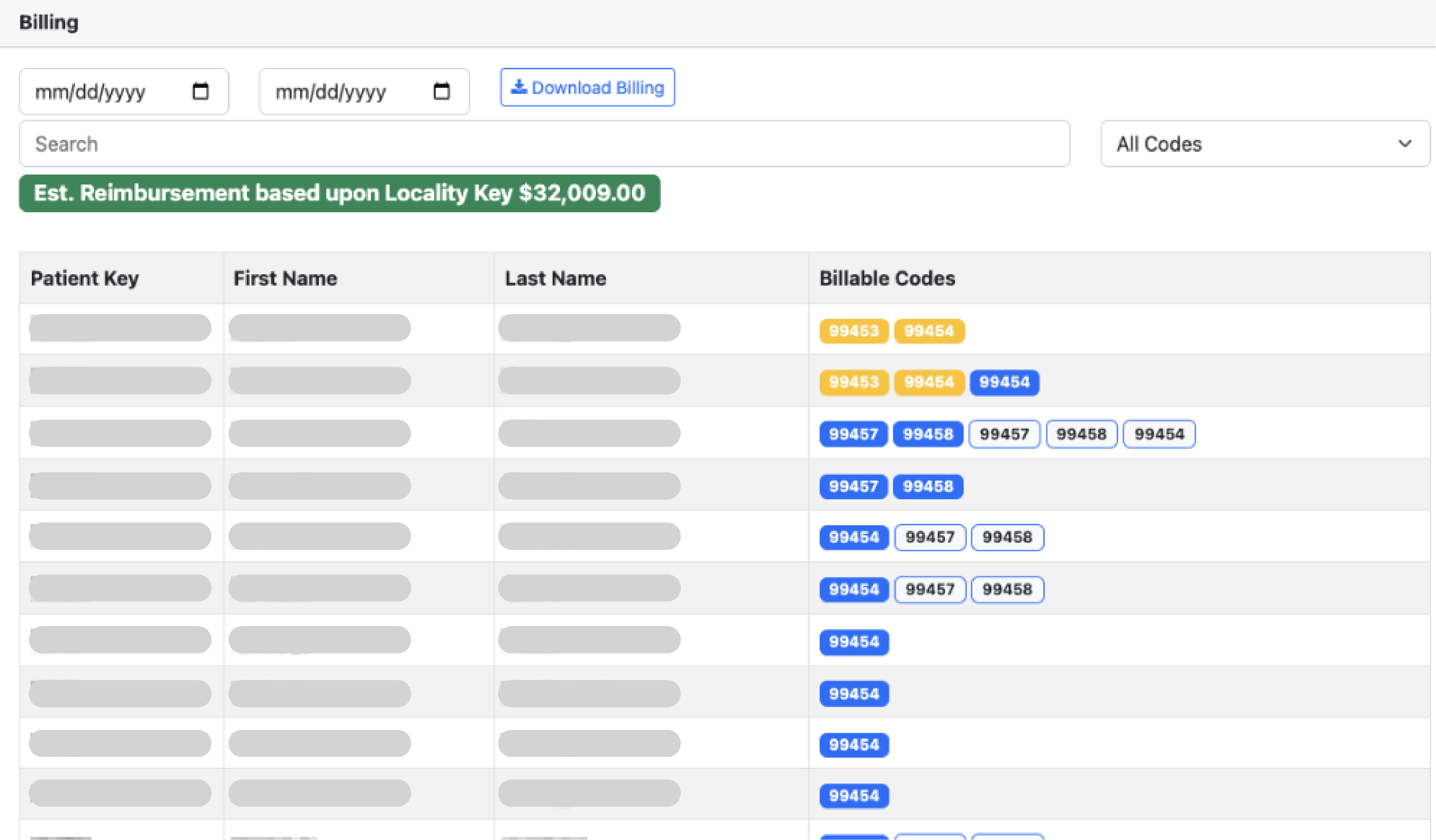
BillingQ: The Pre-Flight Check
Make “Compliance-as-Code” real. BillingQ treats compliance as a systems problem, not a training problem. It encodes the rules so risky claims never make it to your billing team.
- Cross-Program Rules Engine: Understands how RPM, RTM, CCM, and APCM interact. Bundles APCM services correctly and enforces RPM’s structural rules (like 16 days of data) before a period is ever marked for billing review.
- Embedded Regulatory Mapping: OIG red flags and MAC guidance are encoded directly into BillingQ. If a patient hasn’t met thresholds or components, the claim is flagged and prevented from appearing in the “ready for billing review” list by your configured rules.
- Code Stacking & Bundling: Automatically flags conflicting codes (e.g., RPM + CCM overlaps) and ensures APCM bundles meet all service requirements before billing.
- Automatic Time Tracking: Every interaction, including calls, reviews, and messages, is timestamped and categorized automatically, aggregating time toward the correct codes without manual tallies.
Built-In SOPs & Governance
Don't reinvent the wheel. FairPath includes embedded operational procedures for enrollment, review, and QA, refined over millions of patient interactions.
Scalability without Chaos
The same operating model works for 100 patients or 10,000+. Queue-based workflows mean you scale by adding roles, not by rewriting software.
How FairPath Supports Clinical Care
Structured care pathways, AI-assisted drafting, and patient engagement keep clinicians in control as you scale from a few dozen patients to a multi-thousand panel.
The Blueprint: Evidence-Based Pathways
Remote care fails without a roadmap. FairPath provides Ontology-Driven Pathway Schemas that act as the clinical blueprint for your program and support consistent care. Developed in partnership with leading clinicians and refined over millions of patient interactions.
AI-Assisted Drafting & Analysis
Amy (AI) analyzes patient history and comorbidities to draft a comprehensive care plan for you. She suggests goals, phases, and interventions based on your clinical guidelines within a secure, HIPAA-compliant environment.
Draw from our library of best-practice schemas (HTN, Diabetes, COPD), or encode your own proprietary protocols.
Stop juggling separate plans. Create a single CarePlan that manages multiple chronic conditions at once. The system links documented activities to program requirements and shows progress toward common thresholds; payer rules vary and the practice remains responsible for coding.
Track every development. FairPath audits every change to the care plan, creating an immutable history of patient progress and provider decision-making.
Your Clinical Workspace -- Work Only Where It Matters
The Priority Q puts the most important patients in front of you first. Instead of reviewing every reading or bouncing between charts, clinicians work from a single queue of exceptions for critical vitals, worsening trends, and “no data” patterns. AI evaluates incoming readings in real time so you decide how hands-on you want to be, and the software absorbs the rest.
Critical alerts jump to the top. Scheduled follow-ups for CCM and APCM appear automatically when due. Filter by event type or let the AI decide what's next so your effort is defined by clinical need, not panel size.
Watch billing codes track in real-time. As you log time or complete tasks, progress bars fill up instantly so you know exactly when thresholds (like CCM 20 mins) are met.
Call or text patients directly from the chart or queue. Every attempt is automatically logged to the audit trail and contributes to time tracking.
Stop typing. FairPath automatically transcribes and summarizes every phone call. You can also dictate your own clinical notes. Both the original audio and transcript are saved in a HIPAA-compliant archive.
"Amy (AI)" Patient Engagement
Amy (AI) is an embedded capability of FairPath, not a separate product. She handles routine friction so your clinicians can focus on complex care: sending nudges to keep patients on track for RPM requirements (like 16 days of readings), troubleshooting connectivity, and delivering structured symptom surveys via text or voice.

Device Support
Walks patients through fixing connectivity issues to keep data flowing.

Compliance Nudges
Reminds patients to take readings or complete APCM elements.

Surveys & Queries
Collects structured symptom data and answers common questions.

Smart Escalation
Recognizes clinical risk and hands off to human staff with context.
The Operational Shift: You choose how little or how much to personally touch; FairPath ensures that whatever reaches your staff is worth their time, defined by exceptions rather than panel size.
Backed by SemDB and OGAR guardrails to ensure HIPAA compliance and minimize hallucinations.
Why Run RPM at All? Because the Clinical Data Is Real.
When RPM is managed correctly--as part of a thoughtful remote‑care stack--the clinical lift is significant. In a controlled study of 192 chronic‑care patients, structured monitoring delivered:
-
17% Drop in High‑Risk Vitals
Out‑of‑bounds readings dropped from 59% to 42% in just 90 days.
-
Higher Adherence
Daily reading frequency increased by 22% as patients engaged with the feedback loop.
Patient Health Stabilization
Reduction in Out‑of‑Bounds Readings
Due Diligence Briefing
Understanding Third-Party RPM Vendors: Key Considerations
Remote care programs can be run internally or outsourced to a "full-service" vendor. While vendors initially appeared to solve logistical problems, a clear set of structural risks has emerged. The market is actively shifting away from these high-volume "RPM Factories" toward panel-based models like APCM. Before signing or renewing, evaluate your program against these three critical pillars.
The Economic Trap: Revenue Capture
Vendor models are often built on "revenue share," but in practice, they capture the majority of the program's value while leaving you with the denial risk.
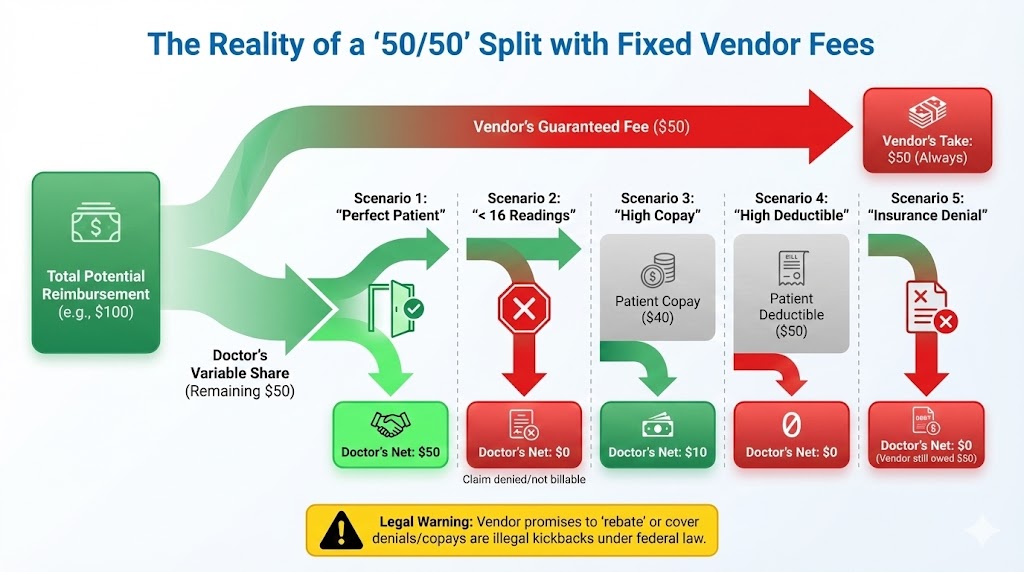
Where the Money Really Goes
When you add device charges, shipping, and administrative fees to a standard revenue share, it is common to see vendors consuming 50–70% of total program revenue.
Persistent Fees: You often owe fees even if patients miss the 16-day threshold or claims are denied.
Device Liability: Hardware costs frequently stay with the practice if devices are lost or unreturned.
“I don’t care if the doctor makes money.”
-- CEO of a leading remote care company, describing their business model
Key Question: What is your realistic net RPM margin after all vendor-related costs across diverse real-world scenarios?
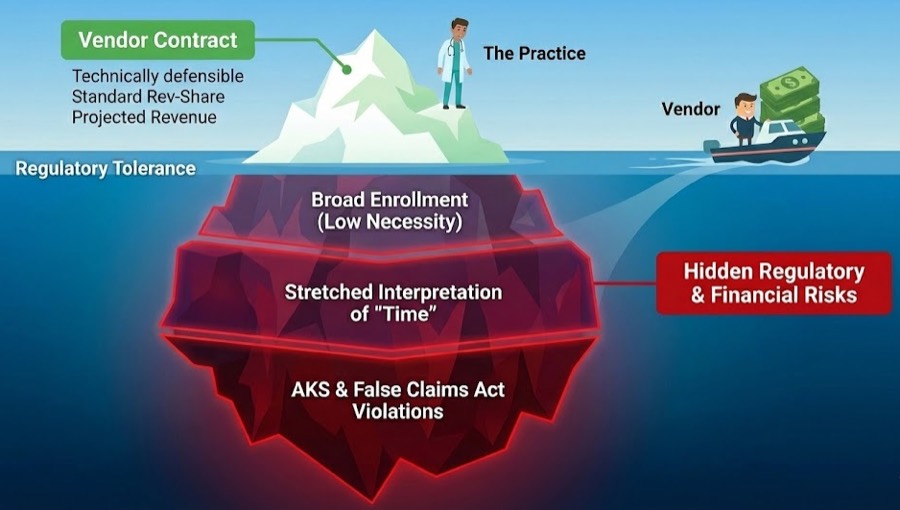
The "Volume Incentive" Loop
When vendor income scales with enrolled patients and billed codes, the incentive tilts toward volume: broad enrollment of "on paper" candidates and a tendency to "stretch" time rules.
AKS (Anti-Kickback Statute)
Concerns about volume-based payments tied to federal program business.
Stark Law & FCA
FCA Risk: If billing systems systematically overstate time, components, or medical necessity.
Split-view graphic.
Left: “OIG Findings” with warning icon (e.g., “43% incomplete”).
Right: “Payer Reaction” with lock icon (e.g., “UHC 2026--Narrowed Criteria”).
The Market Reality: Oversight bodies are responding. The OIG found substantial non-compliance in high-volume programs, and payers like UHC (2026 Policy) are narrowing coverage criteria in direct response. High-volume, vendor-heavy programs now operate under maximum scrutiny.
Regulatory Exposure
A contract can be technically defensible on paper and still push behavior toward the edge of what regulators will tolerate. Ultimately, your NPI is on the claim.
Loss of Control & Strategy
Outsourcing creates a "Black Box" around your data and locks you into a device-centric model just as the market shifts toward comprehensive care (APCM).

Vendor models optimized for RPM hardware margins align poorly with an APCM-first strategy, where RPM is used selectively as a clinical tool rather than a volume driver.
Patient Experience & Data Sovereignty
Vendors often prioritize "clean" claims, leading to the exclusion of complex patients who need care most. Furthermore, because outreach comes from the vendor but looks like it comes from you, aggressive reminders or scripted calls damage your brand.
The "Black Box" Problem
In many vendor models, the complete audit trail lives in their portal. Full, structured exports can be difficult or costly to obtain, complicating any future transition.
- Can you reconstruct who was enrolled and when without their help?
- Do you have raw access to the device logs that support your billing?
- Are there exit penalties or minimums that lock you in?
CMS is actively incentivizing panel-based models like APCM. These models reward ongoing primary care rather than device quotas and naturally align with in-house teams--not with external "RPM factories" taking a percentage of reimbursement.
Summary Checklist: Questions to Ask Before Signing
Don't sign a "full-service" vendor agreement until you have clear answers to these six questions:
Economics
What is our realistic net RPM margin after accounting for all vendor costs, denials, and lost devices?
Regulatory Risk
How do you ensure we receive our revenue split without violating the Anti-Kickback Statute?
Oversight & Liability
Are you willing to assume legal and financial risk if CMS audits and claws back reimbursements?
Patient Equity
How do you deal with patients who have co-pays? Or patients on Medicaid?
Data Control
Can we download a complete, structured export of our data today without a fee?
Contract Terms
What is the specific cost to exit this contract before the 1-year mark?
The Market Is Moving Away From Vendor‑Run "RPM Factories"
OIG’s RPM findings and payer policy changes are not abstract. They are direct responses to the high‑volume, low‑documentation patterns that vendor‑driven models created.
The Headwind: RPM Factories
Regulators are targeting "device quotas" and high-volume billing without clinical context.
- OIG Scrutiny: Flagging claims with minimal device activity.
- Payer Cuts: UHC 2026 narrowing "medical necessity" for devices.
- Vendor Risk: Outsourced models create the exact patterns audits look for.
The Tailwind: APCM + In-House
CMS is actively incentivizing panel-based management models like Advanced Primary Care Management (APCM).
- Panel Stability: Ongoing management rather than device counts.
- Layered Care: RPM/CCM added only where clinically appropriate.
- FairPath Alignment: Our OS is built to run this exact stack in-house.
FAQ
Your RPM, APCM, & Compliance Questions, Answered
These FAQs focus on how a modern, in‑house RPM/APCM/RTM/CCM stack works on FairPath--and how to think about vendors if you’re currently using one.
Will my RPM program be reimbursed for any chronic disease?
No, and this is a critical risk. Payer policies are tightening. UnitedHealthcare’s 2026 policy states RPM is only “necessary” for heart failure and hypertensive disorders of pregnancy, meaning RPM for other common conditions can be denied.
This is why relying only on RPM is dangerous. FairPath integrates Advanced Primary Care Management (APCM), a CMS‑approved program with stable, predictable revenue that isn’t diagnosis dependent. We help you build durable APCM revenue and layer RPM where it is both clinically appropriate and financially secure.
What if my RPM vendor handles everything but takes a large revenue share?
This is the “Vendor Trap.” That 50–70% rev‑share erases your margin.
The Math: You bill $100. They keep $70. You keep $30.
The FairPath Model: You bill $100. You pay a simple software fee. You keep the rest.
We stay transparent, while rev‑share vendors obscure true practice profit and push billing patterns that leave you holding the liability. FairPath provides the operating system; you keep the revenue you earn.
Do we have to change our EMR or add a new system?
No. FairPath sits alongside your existing EMR. We integrate with your current workflows so your team doesn’t have to relearn everything or juggle another core system.
How do I handle billing and audit readiness? I’m worried about denials.
Stop trying to do it manually. FairPath’s Compliance‑as‑Code engine prevents bad claims before they are submitted by:
- Running a “Pre‑Flight Check” on every claim against OIG and MAC‑specific rules.
- Preventing code‑stacking conflicts (e.g., RPM vs. CCM/APCM overlaps) automatically.
- Monitoring the 16‑day transmission requirement and alerting you before the month ends.
- Generating an immutable audit trail so you can defend every claim.
Your staff doesn’t have to memorize billing rules--our software already knows them.
How do I evaluate leaving my RPM vendor for a software‑based model?
Start by requesting two things: a complete patient data export and the exit fee. Vendors that resist either are signaling lock‑in.
We are the anti‑vendor. FairPath is built on 100% Data Sovereignty. From day one you have full access to patient lists, device logs, and claim history, and you can export them anytime. Use the RPM Vendor P&L Analyzer and our Exit Blueprint to understand both the economics and the operational path out.
How do I handle device costs and logistics?
You take back control. Rev‑share vendors often lock you into pricey hardware leases to create hidden margins.
FairPath is device‑agnostic. We integrate with low‑cost commodity hardware and support patient‑owned devices where appropriate so you can reduce overhead and keep the margin you earn--without making hardware a new point of lock‑in.
How will payer policy changes affect my practice in the future?
Payer policy will change, and it will be disruptive. UHC’s 2026 update proves RPM‑only programs sit on unstable ground.
FairPath is a multi‑program platform that centralizes RPM, RTM, CCM, and especially APCM. When payers tighten RPM, you can pivot to APCM instead of watching revenue collapse. Our goal is to keep your practice stable, diversified, and ready for whatever comes next. If you want to understand the APCM‑first model in detail, read our APCM‑First strategy guide →.
How long does it actually take to move off our RPM vendor?
Plan on 60–90 days. We start by stabilizing your current panel, then run FairPath alongside your vendor so you can validate eligibility scoring, PriorityQ, and BillingQ against their work. Once the data and payouts match, we wind down the vendor contract--without forcing you to hire new staff.
Ready to Design RPM and APCM on Your Own Terms?
Whether you are just exploring remote‑care options or actively evaluating a vendor, you don’t have to guess. See how FairPath would run your stack, and benchmark your current model against a software‑driven, APCM‑first approach.
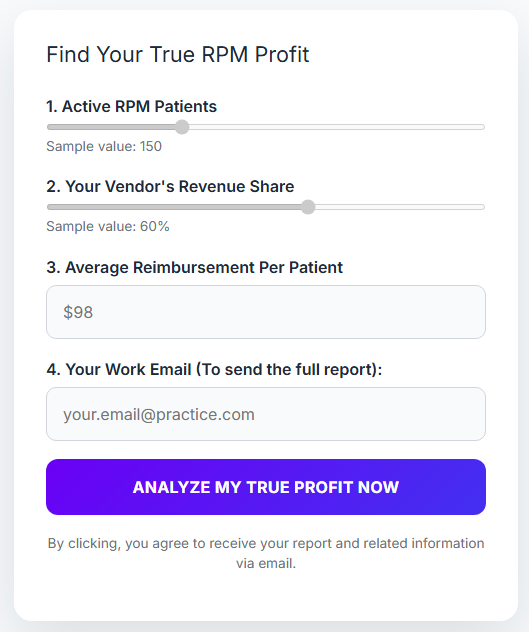
Your Numbers Are Unique.
See Them Now.
The RPM Vendor P&L Analyzer takes "we’re probably getting ripped off" and turns it into hard numbers. Enter your vendor, patient count, and rev-share to see:
- Line-by-line breakdown of what you earn vs. what they keep.
- Risk detection for device-day gaps and code stacking.
- Exact comparison of your margin on a software-fee model.
FairPath Is the Remote-Care OS for Practices
Not another vendor. The software you use to replace the vendor.
Multi-Program Spine
Runs APCM, RPM, CCM, and RTM on one integrated platform.
Compliance-as-Code Engine
Eligibility scoring, Amy (AI Assistant), PriorityQ, and BillingQ automate the work.
100% Data Sovereignty
Works alongside your EMR under your governance. Your data, always.
FairPath works alongside the EMR you already use: