CMS has fused APCM eligibility, practitioner attribution, and continuity into a single monthly operating system. Billing without that coherence now creates denial and audit exposure. If you are treating these as three separate checkboxes, you are already behind.
We just published a full operational guide on APCM eligibility, attribution, and continuity that explains how CMS now treats them as one system and what you need to reconcile inside each billing month. Below is a practical breakdown of what it means and what to do next.
The Core Shift
APCM is not a code you bill because a patient is "eligible." It is a monthly bundle that requires eligibility, attribution, and continuity to all reconcile inside the same billing month. CMS is paying for longitudinal ownership of a patient's primary care, not for isolated events.
That means:
- Eligibility must be true in the billing month (not just at enrollment)
- Attribution must be valid (the named practitioner who bills APCM must be the one providing continuity)
- Continuity must be evidenced (care plan access, touchpoints, 24/7 availability)
If any one of these fails for a given month, the APCM claim is not defensible.
The Practical Risk
The most common failure mode is billing APCM based on enrollment status without verifying month-specific evidence. A patient was enrolled in January, so the practice bills APCM every month without checking whether the care plan was updated, whether the attributed practitioner is still the one providing care, or whether continuity was maintained.
That is the kind of gap that auditors find immediately. And with the OIG's 2026 RPM and care management audit cycle underway, the exposure is not theoretical.
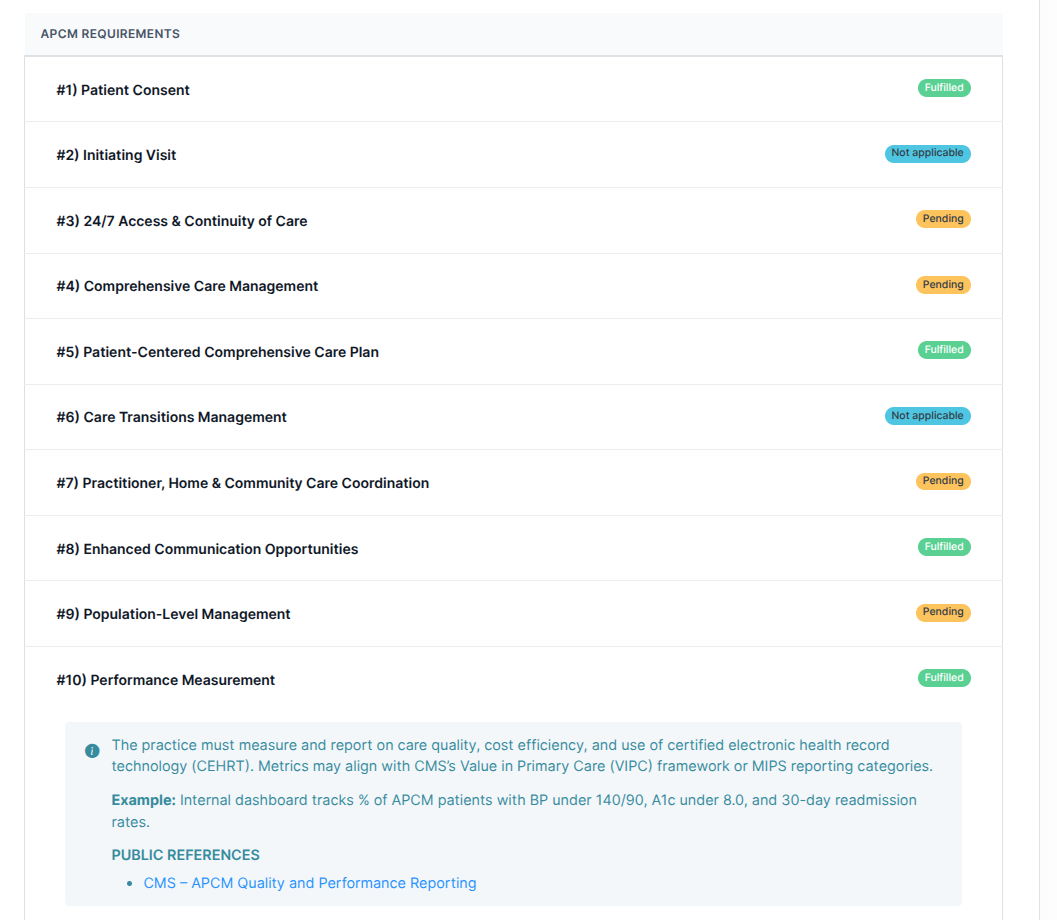
What You Need Each Month
- Valid eligibility (patient meets APCM criteria for the billing month)
- Attribution integrity (the billing practitioner is the one providing continuity)
- Care plan access and review evidence (a lightweight monthly attestation can satisfy this when no major edits are needed)
- 24/7 access and continuity documentation
- Communication and care coordination logs
- Separate evidence streams if you are also billing RPM, RTM, or behavioral health add-ons
The Bottom Line
APCM is a monthly operating system, not a one-time enrollment. If your workflow does not reconcile eligibility, attribution, and continuity every month, you are baking denials into your revenue model. The fix is not more work - it is the right workflow with the right checks at the right time.
The full guide with the CMS framework, FAQ, and operational checklist is at APCM Eligibility, Attribution, and Continuity: One System.
Related resources: Advanced Primary Care Management (APCM) Guide, APCM Bundle Rules: When CCM/PCM Must Stay Off the Claim, APCM Reporting Guide.
Disclaimer: This article is informational only. Coverage, coding, and rates vary by Medicare Administrative Contractor (MAC) and payer plan. Confirm payer-specific requirements with your billing team or counsel.